
A first year medical school report by Kirsty Mackenzie, University of Dundee, written as part of a Student Selected Component (SSC) on Human Factors (March 2018). This is also available as a PDF.
Introduction
Over the past century and particularly over the last few decades, there has been a huge shift in the way in which patients interact with doctors. In the past, patients were given very little information about their conditions or their treatments. Medicine was very paternalistic and there was little room for patients to question the doctor’s decisions or to make choices for themselves. The public had very little scientific knowledge and blindly agreed to treatments that may not have needed or wanted(1). This was not in the best interests of patients because they had no control over their own health and this must have left them feeling less content and more anxious about what they were going through. The old model of ‘doctor knows best’ has in recent times been put aside in favour of ‘person-centred care’. The Royal College of Nursing states ‘[Person centred care] means that the person is an equal partner in the planning of care and that his or her opinions are important and are respected(2).’ This term was first coined by the psychotherapist Carl Rogers building on earlier ideas proposed by healthcare workers. Further building on Rogers’ ideas, the psychiatrist George Engel promoted ‘the move from a medical to a biopsychosocial the move from a medical to a biopsychosocial model of health(3).’ His ideas have been widely credited with being responsible for the shift in the model of care.
More recently, the Mid Staffordshire scandal, where according to the Guardian ‘disputed estimate suggested that between 400 and 1,200 patients died as a result of poor care over the 50 months between January 2005 and March 2009 at Stafford hospital(4),’ led to a significant change in policy in the NHS. In NHS England, this was through the Health and Social Care Act of 2012(5) and in Scotland this is still ongoing as part of the ‘2020 Vision’ Quality Strategy. One of the ‘quality ambitions’ of this strategy is to form ‘Mutually beneficial partnerships between patients, their families and those delivering healthcare services which respect individual needs and values and which demonstrates compassion, continuity, clear communication and shared decision-making(6).’ Part of this shift to shared decision making has been put in progress by improving patients’ access to information- through leaflets, websites, apps and better conversations. This report will focus on the use of leaflets to educate and inform patients. Treating patients as people and as partners in their own treatment improves patient satisfaction(7) and also makes their treatment far more ethical. This is because medical ethics are based on principles of respect for autonomy, beneficence, non-maleficence, and justice(8). The old order of medicine did not show any respect for autonomy and could not have guaranteed beneficence without properly talking to the patient and asking what they thought was best for their own health.
Patient information leaflets (PILs) serve several purposes- some are found in medication boxes and inform patients about the drugs they are taking, others are made by health providers and inform about conditions, treatments and procedures so that patients are better informed about their own health, others are more for the general public and give information about maintaining good health, screening programmes or vaccinations. All the leaflets are designed to educate patients and help them be more active in making decisions about their treatment. They are representative of the increasing role of patients in their own healthcare- the progression of laws around medication PILs shows this very clearly. The first laws around PILs were made in 1977, at which point most medications did not come with any information. Most of those that did were inhaler administered medications that required technical explanations of how to use them. By 1994, a European Commission-issued directive to ‘to give users full and comprehensible information’ had been incorporated into UK legislation. This led to the blanket provision of PILs in all medicine packs by 1999 and the Medicines Control Agency produced a guidance document for drugs manufacturers meaning that the information provided could be given in a standard form and would theoretically be within the bounds of most peoples’ literacy level.
The NHS has produced a guide on the best practice in producing a PIL and has made templates for different formats of leaflet, making the design of leaflets more standardised and less amateurish(9). The time and effort put into this fairly exhaustive guide show the importance of these types of resources in the everyday running of the NHS.
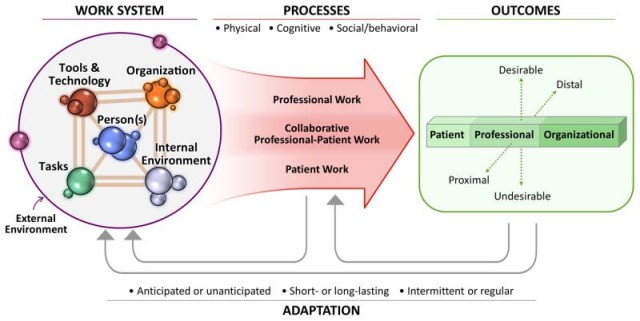
Human factors are defined as ‘Enhancing clinical performance through an understanding of the effects of teamwork, tasks, equipment, workspace, culture and organisation on human behaviour and abilities and application of that knowledge in clinical settings(10).’ Human factors have three core principles – 1) systems orientation, 2) person-centredness, 3) design-driven improvements (Appendix 1) (11). These principles are used to help see the ways in which a system can be improved in order to increase safety, patient satisfaction and efficiency. The Systems Engineering Initiative for Patient Safety (SEIPS) model(11) is a framework which links work systems to processes and outcomes and promotes improvements to the way healthcare is delivered, especially person centredness. PILs could be viewed as tools used by the patient in the work system which help them in their internal environment to think over their options and make decisions. The SEIPS model is a useful way to set out the principles of Human Factors in a way that directly links together the elements of the system around each patient.
Benefits of Patient Information Leaflets
Giving a patient a PIL immediately gives them the opportunity to participate in their own care. With the information they can gain from a leaflet, a patient can understand their diagnosis, treatment and/ or prognosis with much more clarity and can make informed decisions. Consent will be given with more certainty and more ethically. In a short consultation, it is often challenging to give a patient all the information they need to make a decision. The NHS choices website gives the average length of a GP consultation as 8-10 minutes(12), a very short slot of time if discussion, examination and management are to be fitted in. Additionally, even if the doctor does manage to convey all of the information to the patient, it is unlikely that the patient will fully take it all in at the time. This is especially true if the patient has just been given difficult or upsetting news, as they may ‘zone out’ and stop listening to the doctor. Giving a PIL means that the patient can read the information in their own time and gives them time to assimilate it.
Increased education of patients is also important in increasing their satisfaction with their treatment. It is not always possible for a doctor or nurse to sit down with the patient and fully explain what they are going through, but one of the main factors that patients stated in an American study as increasing their satisfaction with time spent in the Emergency Room was the amount of information nurses gave them about what was happening to them(13). Therefore, if the use of patient information leaflets allows increased knowledge for patients even when staff do not have time to talk for extended periods, satisfaction should be increased. An older study looking into the effect of PILs giving information on Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), beta blockers and inhaled bronchodilators showed that patients who received the leaflets were significantly more satisfied with their care than those who did not(14). Despite the age of this study (30 years old), the information provided was about drugs that are still in very common usage today. The passing of time will have decreased its usefulness to some extent, but there is still much information to be gleaned from its findings.
The same study yielded results which showed that patient awareness of the benefits and side effects of their medication increased after reading the leaflets. They also took their medicines more effectively which had the potential to cause better outcomes. A systematic review of studies on inhaler technique errors also reflected this trend, stating ‘ inhaler technique interventions were found to decrease error frequency, and have positive impacts on disease and patient outcomes’(15). A similar effect can be seen in another study looking into the effect of PILs on antibiotic prescription frequency. It found that leaflets on common infections led to lower re-consultation rates and fewer antibiotic prescriptions(16). This is because again the leaflets had educated the patients on why antibiotics should only be used in certain infections. They also had the potential to improve outcomes for both the patients and those around them by reducing the risk of resistance to the antibiotics forming.
Issues with Patient Information Leaflets
PILs should always be used in conjunction with discussion with a health professional, they should not replace face to face communication. If they did, this would remove one of the most important elements of the SEIPS model- the patient-professional relationship- and make the process of treatment less effective. There is also some evidence that patients prefer to talk to a doctor than read a leaflet, which is unsurprising(17).
One of the main problems about the leaflets is that many are not easy to understand, especially to those with lower levels of literacy. A study of three PILs found that none of the leaflets achieved the European Guideline of 80% as a success score in whether the patients could read and understand the information given to them(18).
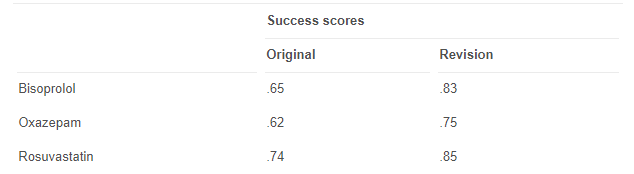
These findings show that the information being provided to patients is falling short of requirements and is therefore much less useful to patients. On adapting the leaflets to make them more readable, two of the leaflets increased their success scores to above the guideline, but one failed to meet the guideline. This suggests that making leaflets easier to understand is a difficult process. The ideas being conveyed in the leaflets may be complex and therefore challenging to present to the average person.
Another issue is that many patients will have low levels of literacy and education in general, leading to them having difficulty understanding written information. Face to face communication may be the only way to get information across to patients because they will simply not have the ability to read a leaflet. One study found that despite the average reading ability of an American being 7th grade level (12-13 years old), the majority of a randomly selected sample of online patient information was of a ‘difficult’ reading level (9th grade (14-15 years old) or above)(19). Considering that the World’s Most Literate Nations (https://www.ccsu.edu/wmln/) found that the UK is the 17th most literate country in the world, lagging 10 places behind the USA at number 7, the study gives a concerning picture of the effectiveness of PILs, though PILs may be pitched at a higher level in the USA.
It is also easy enough for a patient to have preconceived misconceptions about their health or medical concepts. A review of papers on patient health literacy for the Royal College of Surgeons found that misconceptions of common medical terms are a serious problem in healthcare. For example, a 2006 study found that ‘84% [of patients] thought there was a difference between a fracture and a break, with 68% believing a break to be worse than a fracture(20).’ Another study reviewed in the article found that ‘many patients in an emergency department were unable to match words such as haemorrhage and bleeding or heart attack and myocardial infarction.’ Yet another study found that ‘Alarmingly, 45% of patients with hypertension and inadequate health literacy did not know that a blood pressure of 160/100 mmHg was high.’ These findings show the low understanding of basic medical concepts, even those pertaining to patients’ own conditions. Doctors assume that patients understand when hearing these apparently simple terms but lots of information can be missed if the patient does not have any basic medical knowledge. This is particularly relevant when writing a PIL because it completely relies on the patient having a certain level of literacy. Reliance on PILs without considering the appropriateness of the resource to a patient can potentially be dangerous, as shown by a study which found that ‘up to 78% of patients with low literacy misinterpret warnings on prescription labels’(20). Deprivation is strongly associated with low health literacy, a study found that when deprivation and income are used together in analysis, those in the most deprived areas were more than twice as likely to have limited health literacy. Therefore, the high reading ability needed to read PILs widens health inequalities by giving more health literate and likely more privileged people more information about their treatment.
A significant problem with the PILs provided by the NHS is their inconsistency. Despite specific guidelines being developed by experts in their fields around advice for patients, some health trusts, local authorities and individual doctors produce their own resources. These can contradict each other, provide incorrect information and lead to confusion for patients. A survey of the instructions provided to patients after inguinal hernia repair surgery found that the time to wait before resuming certain activities had a very wide range- for example the recommended time to wait before driving ranged from 24 hours to 6 weeks and the time to wait before resuming playing sports ranged from 2 weeks to 12 weeks(21). This discrepancy is both unhelpful and unnecessary. It could be avoided by following guidelines produced by the Royal College of Surgeons which give the best practice for care after this specific surgery(22). These guidelines state that ‘Normally, you should refrain from driving for at least 1 week after a hernia repair operation.’ Clearly this is contradicted by some of the leaflets looked at in the study and could lead to dangerous situations for both the patient and other people on the roads. The guidelines strongly suggest that patients should be off any strong painkillers and undistracted by pain before they can drive, and this seems highly unlikely 24 or even 48 hours after surgery. Work is needed to standardise leaflets across the many trusts and authorities in the UK so that the information given is as accurate, up-to-date and useful as possible.
There is evidence that PILs, far from alleviating concerns, can increase anxiety. This is strongly associated with ‘information overload’- defined as ‘the situation when someone has so much information that they are unable to deal with it’(23). The study found that in a group of university students, the more effort they had to put into reading the leaflets, the higher the levels were of information anxiety, confusion, doubtfulness and frustration. The subjects of the study, being university students, were presumably reasonably well educated, with higher levels of literacy than the average patient. Considering the level of literacy required to read many of the PILs in the study previously discussed, it can be assumed that leaflets frequently lead to anxiety and failure to read the information at all. This is a big problem because it leads to a lack of education for the patient and makes it less likely that they will use the medication properly. An issue with the study was that the subjects used were much younger than the normal target audience. However, when discussing the limitations of their study, the authors stated ‘one could note that if young adults found the information overloaded, one would expect the elderly, who are typical consumers of prescription medications, to have a more pronounced effect’(24). Therefore, the increased levels of anxiety found in the students would probably be exceeded in real patients.
Ways to improve Patient Information Leaflets
PILs can be highly useful resources, but only if they are used sensibly in conjunction with talking to a health professional. There is clearly a lot of room for improvement in how they are written and laid out, as well as the information they provide. PILs exist as a tool in the SEIPS model for patients to use to improve their experience of treatment. In the model, people are said to be influenced by the tools and technology, organisation, tasks and their own internal environment, as well as their external environment. Together, these factors make up the work environment in the system and govern what the patient’s experience through work processes will be like.
A crucial way in which patient experience of information leaflets could be improved is for the organisation component of the system to be refined. If groups involved in the same processes in different hospitals and authorities came together and standardised the information given to patients, this would be highly beneficial. Local authorities and health trusts with good patient information could share their expertise and help less well organised counterparts to better coordinate their advice and make it more accessible. Better protocols of how and when to give information could be discussed and again standardised across the board. Some organisations are better at informing patients than others. For example, Guy’s and St Thomas’ NHS Foundation Trust produces its own leaflets, there are around 850 of them and they are all available for free online. Clinicians and health professionals write them, meaning the information is up to date, accurate and not lifted from elsewhere(25). Patients test them out so that it is ensured they are easily read and understood. Often, concerns of cost are the issue but Guy’s and St Thomas’s Director of Communications, Anita Knowles said of the trust’s decision that ‘it was just as cheap to do it ourselves.’ Despite this, it would perhaps help the system organisation if more funds were made available to research and produce high-quality information.
It seems that much of the difficulty patients have with reading PILs is down to issues with format. A Danish study found that of 111 patients who completed a survey on their ease of reading a leaflet, 38% had difficulty. Interestingly, 57% of these people attributed their issues reading the leaflet to text size, compared to only 33% who found the written language difficult to understand. Particularly in older patients, it may be extremely beneficial if text size is increased. Other suggested measures from the study on information anxiety(24) include ‘chunking, segmentation, pictures, and colors[sic]’ as well as ‘simple illustrations… tied to simple, understandable words.’ These methods of improvement are very much about the design of the information rather than the content and aim to aid less literate patients in their understanding. The process of improving the leaflets in this way strongly feeds back into the principles of Human Factors. The leaflets are written in a more considered, patient centred way, leading to improved outcomes and decreased time needed for doctors to explain concepts to patient. This improves organisation and efficiency, meaning the limited resources of the NHS can be used more effectively.
The idea of involving patients in the process of producing the information also very much feeds into the ideas of the SEIPS model. Patient and Professional-Patient Work are placed on the same level in the model as Professional Work. It doesn’t matter how well the professional thinks they have done in providing information- if the patient does not understand it, there is little value in putting money into producing the leaflets. Human Factors stress that tools and resources used by patients should work around patients and not the other way around. New methods to produce better PILs have included patients in the design of the materials. European Commission Guidelines on PILs for medication boxes (26) state ‘Articles 59(3) and 61(1) of Directive 2001/83 require that the package leaflet reflects the results of consultations with target patient groups to ensure that it is legible, clear and easy to use and that these results of assessments carried out in cooperation with target patient groups are also provided to the competent authority.’ One way which they suggest doing this is user testing- giving patients leaflets in development and asking them questions about their understanding of the information and how easy it is to read. Therefore, some hospitals are already within these standards, but many have a long way to go before meeting requirements.
A novel way of increasing readability of PILs is to let children design them. In 2017, 57 children, aged 8-10 were educated about the ‘anatomy, technique, and indications for and risks associated with total hip arthroplasty’ and asked to write their own patient information leaflets(27). They were also allowed to draw a picture relating to the surgery. The children were very receptive to the idea and enjoyed the experience, leading to more interesting, engaging and easy to read leaflets. The study was not particularly serious and did not test out the leaflets on patients, but showed a new insight into the level of literacy that the average person has- that of a 9-year-old. This idea could potentially be useful as a means for making more helpful and fun leaflets. Some of the results are shown below (Figures 3 and 4).

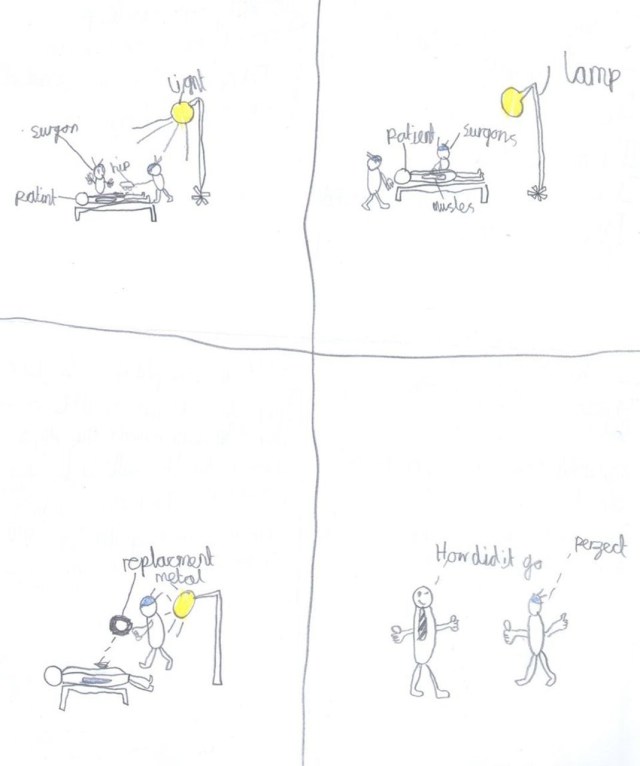
The study was less about the resources reduced and more about the ability of the patients that leaflets are aimed at. Though very precocious for their age, the children focused on information that would not normally be found in a leaflet and their drawings were striking in their innocence. If this is the level of ability that the average patient has, the leaflets that the children produced may be more appropriate than the jargon-heavy, information-dense resources that are taken as normal.
Conclusion
Patients’ involvement in their own care has increased substantially since the days when ‘doctor’s orders’ were non-negotiable. Doctors now give options to the patients and discuss what would be best for them. Patient information leaflets have been important in giving patients the opportunity to assess their options and assimilate what they may go through in their treatment. This is especially important due to the short amount of time that doctors often have to talk to patients. Educating patients can also lead to better outcomes, as they make fewer mistakes with taking medications and know what to expect. However, there are lots of issues with the quality of resources on offer, reducing their usefulness. Some are inconsistent, inaccurate and difficult to read, which is a problem because the patients who are given them often have low literacy, specifically low health literacy. The shortcomings in the leaflets mean that health providers are missing out on a valuable method of improving outcomes. If more engaging, easier to read leaflets were produced with input from patients, the value of the information provided to patients would increase. There are already guides in existence which could help with the improvement process but more work will be needed, since even with the use of European Commission Guidelines, many patients struggle to understand the information given to them(18). Use of novel techniques, including those involving working with children, could help with speeding up the process of improvement. With increased funding and some time and effort, patient information leaflets could become extremely helpful.
Appendix 1
- Principle 1, Systems orientation. Performance results from the interaction of a sociotechnical system in which the person is but one embedded component (this has motivated healthcare to replace a blame-the-person culture with a more holistic system-based approach).
- Principle 2, Person-centeredness. The person, or group of people, is central in a healthcare work system, meaning that efforts must be taken to support people through the design of work systems that fit their capabilities, limitations, performance needs, and other characteristics, not the other way around.
- Principle 3, Design-driven improvements. Person-centered design of work structures and processes, when grounded in sound human factors science and practice, can improve myriad important patient, provider, and organizational outcomes.
References
- Robb M. The end of paternalism? [Internet]. Vol. 10, Nursing management (Harrow, London, England : 1994). 2004. p. 32–5. Available from: https://www.medicalprotection.org/uk/advice-booklets/mps-guide-to-ethics—a-map-for-the-moral-maze/chapter-1—ethics-values-and-the-law/the-end-of-paternalism
- Royal College of Nursing. First Steps – What person-centred care means [Internet]. 2015. Available from: http://rcnhca.org.uk/sample-page/what-person-centred-care-means/
- The Health Foundation. Person-centred care made simple Quick guide. 2014. 40 p.
- Campbell D. Mid Staffs hospital scandal: The essential guide [Internet]. The Guardian. 2013. p. 1–5. Available from: http://www.theguardian.com/society/2013/feb/06/mid-staffs-hospital-scandal-guide
- National Health Service England. Health and Social Care Act 2012 [Internet]. 2012. Available from: http://www.legislation.gov.uk/ukpga/2012/7/introduction/enacted
- Women’s NL. Quality Strategy [Internet]. 2015. Available from: http://www.liverpoolwomens.nhs.uk/Library/about_us/Quality_Strategy_2014-2017.pdf
- Robbins JA, Bertakis KD, Helms LJ, Azari R, Callahan EJ, Creten DA. The influence of physician practice behaviors on patient satisfaction [Internet]. Vol. 25, Family Medicine. 1993. p. 17–20. Available from: https://www.ncbi.nlm.nih.gov/pubmed/8442550?access_num=8442550&link_type=MED&dopt=Abstract
- Gillon R. Medical Ethics: Four principles plus attention to scope. Vol. 309, British Medical Journal. 1994. p. 184–8.
- NHS. Toolkit for producing patient information. 2003;1–27. Available from: http://www.fundsis.org/docs_act/109_patientinfotoolkit%5B1%5D.pdf
- National Quality Board. Human Factors in Healthcare Patient Stories. Natl Qual Board. 2013;(November):1–22.
- Holden RJ, Carayon P, Gurses AP, Hoonakker P, Hundt AS, Ozok AA, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics [Internet]. 2013 Nov;56(11):1669–86. Available from: http://www.tandfonline.com/doi/abs/10.1080/00140139.2013.838643
- NHS Choices. GP appointments – The NHS in England – NHS Choices [Internet]. NHSchoices. 2016. Available from: https://www.nhs.uk/NHSEngland/AboutNHSservices/doctors/Pages/gp-appointments.aspx
- Bursch B, Beezy J, Shaw R. Emergency department satisfaction_ what matters most_ – PubMed – NCBI [Internet]. 1993. Available from: https://www.sciencedirect.com/science/article/pii/S019606440581947X?via%3Dihub
- Gibbs S, Waters W, George C. The benefits of prescription information leaflets (2). Vol. 28, British Journal of Clinical Pharmacology. 1989. p. 345–51.
- Usmani OS, Lavorini F, Marshall J, Dunlop WCN, Heron L, Farrington E, et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes [Internet]. Vol. 19, Respiratory Research. 2018. p. 10. Available from: https://respiratory-research.biomedcentral.com/articles/10.1186/s12931-017-0710-y
- P M de Bont EG, Alink M, J Falkenberg FC, Dinant G-J, L Cals JW. Patient information leaflets to reduce antibiotic use and reconsultation rates in general practice: a systematic review.
- Horwitz A, Reuther L, Andersen SE. [Patient information leaflets seen through the eyes of patients in a general practice]. Ugeskr Laeger. 2009 Feb;171(8):599–602.
- Pander Maat H, Lentz L. Improving the usability of patient information leaflets. Patient Educ Couns [Internet]. 2010;80(1):113–9. Available from: http://dx.doi.org/10.1016/j.pec.2009.09.030
- Walsh TM, Volsko TA. Readability assessment of internet-based consumer health information [Internet]. Vol. 53, Respir Care. 2008. p. 1310–5. Available from: https://www.ncbi.nlm.nih.gov/pubmed/18811992
- Kyle S, Shaw D. Doctor–patient communication, patient knowledge and health literacy_ how difficult can it all be_ _ The Bulletin of the Royal College of Surgeons of England [Internet]. 2015. Available from: https://publishing.rcseng.ac.uk/doi/full/10.1308/rcsbull.2014.96.6.e9
- Grewal P. Survey of post-operative instructions after inguinal hernia repair in England in 2012 [Internet]. Vol. 18, Hernia. 2014. p. 269–72. Available from: https://link.springer.com/article/10.1007/s10029-013-1075-x#Sec4
- Cash H. Get well soon. Policy [Internet]. 2011; Available from: https://www.rcseng.ac.uk/patient-care/recovering-from-surgery/groin-hernia-repair/
- Collins English Dictionary. Information overload definition and meaning _ Collins English Dictionary. 2018.
- Bapat S, Patel H, Sansgiry S. Role of Information Anxiety and Information Load on Processing of Prescription Drug Information Leaflets [Internet]. Vol. 5, Pharmacy. 2017. p. 57. Available from: http://www.mdpi.com/2226-4787/5/4/57
- McCartney M. Patient information leaflets: “a stupid system” [Internet]. Vol. 347, BMJ (Clinical research ed.). 2013. BMJ 2013;347:f4748
- Commission E. Guideline on the Readability of the Labelling and Package Leaflet of Medicinal Products for Human Use. – [Internet]. 2009;(September 1998). Available from: https://ec.europa.eu/health/sites/health/files/files/eudralex/vol-2/c/2009_01_12_readability_guideline_final_en.pdf
- Wigley C, Bucknall V, Fleming S. Santa’s little helpers: a novel approach to developing patient information leaflets. BMJ 2017;359:j5565
I declare that this report is my own work and that all the references sourced have been seen by me.
Kirsty Mackenzie
27/3/18
