Summary: This blog presents a summary of Quality Improvement methodology and applies it to a question highly relevant to General Practice – how to move away from same day appointments as Covid-19 lockdown loosens, but without overwhelming services. It focuses in on mental health – with an example sequence of PDSA cycles solely for illustrative purposes. It shows how a series of patient encounters (in this case calls to reception to make GP appointments) represents an opportunity for rapid testing, developing an approach that meets the needs of patients and potentially taking pressure off GPs while also providing more patient centred care. The ideas are presented for discussion rather than as a fait accompli. In real life the process of scoping and running a QI project with a team throws up lots of surprises and shakes a lot of assumptions.
I wrote this blog while reflecting on recent discussions with colleagues in a number of settings. It is presented here as a “think piece”, and will hopefully generate discussion in the comments box below. What are your experiences of using QI methods in general practice and other clinical settings?
Dr Graham Mackenzie GP specialty trainee, year 3 of training
Introduction: When it became clear in February and March 2020 from reports from China and Italy that Covid-19 was going to have a major impact on healthcare in the UK, health boards, hospitals and GP practices had to make major changes to the way that they arranged their services. Assessment centres for patients with Covid-19 symptoms were set up. Hospitals discharged unprecedented numbers of patients and cancelled elective operations. GP practices moved mainly to telephone triage, with changing availability of face-to-face appointments as the year progressed. GP practices changed the layout of surgeries, sometimes with considerable structural changes to establish “red zones”. There were also changes to prescribing arrangements and the care of patients with long term conditions.
All members of the GP practice team were affected by the upheaval resulting from Covid-19 with, for example, profound changes for reception staff in the ways that appointments were booked. Some surgeries removed the ability to book future appointments, requiring that patients phoned up on the day, with phonelines opening to bookings at 08:00. This daily “first come, first served” approach was introduced to allow urgent problems to be identified and prioritised each day and avoid future clinics becoming booked up days and weeks in advance with routine matters. The new approach meant, however, that patients with less urgent problems also had to call each morning at 08:00 to stand a reasonable chance of securing an appointment. The approach has had a mixed reception, with some patients unable to call at 08:00 (e.g. if working), and other patients reporting the need to phone over multiple days to arrange an appointment. The system may also put off patients from calling, “not wanting to bother the doctor”, potentially delaying the identification of important medical problems. These issues are not new – there has been a mismatch between need and demand in healthcare stretching back to the beginning of the NHS and beyond. Many of these challenges have simply been amplified by Covid-19.
In March 2021, following two sustained waves of Covid-19 infection in the UK, 3 months into the nationwide Covid-19 vaccination campaign, and with announcements from UK and Scottish politicians spelling out a loosening of lockdown rules over coming weeks and months, GP practices are once again reviewing their working arrangements. This will not be a wholesale return to “business as usual”. There will be aspects of current working that GP practices and patients will want to keep (e.g. some continued availability of telephone consultation). There will be important decisions to make about patient and staff safety in re-opening areas of GP practices to face-to-face appointments, which are likely to take many months to initiate as we monitor Covid-19 figures with the stepwise loosening of lockdown. The appointment systems described above are arguably more amenable to more rapid change, potentially identifying ideas to test over coming weeks, ideally introducing greater flexibility for appointment booking over coming months. Quality Improvement (QI) methodology provides opportunities to identify and test ideas.
Quality Improvement (QI): In brief, QI is an approach that allows us to take a big seemingly unanswerable question (e.g. how to allow the NHS to meet demand), break it down into bitesize chunks (e.g. tailoring appointment system in GP practices), and testing ideas rapidly. This can be summarised as “Think big, start small, test fast” (adapting the motto of the Mayo Clinic Center for Innovation). There are other ways to think about QI work – it should be about working smarter not harder, with a focus on improving quality and outcomes but minimising negative unintended consequences. Is has clear relevance to GP work, which already has such considerations built into the GP contract.
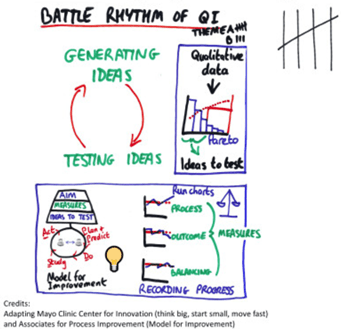
A structure for QI work is provided by the Model for Improvement (Associates for Process Improvement). There is a rhythm to QI work (figure 1) – generating ideas through collection of data through existing processes, and testing ideas through rapid cycle testing (plan and predict, do, study, act (PDSA) cycles).
Generating ideas can emerge from taking a tally – for example from thoughts raised in discussion at a team meeting, or from reception staff or GPs jotting down types of enquiry. If we asked reception staff what the main types of call were likely to be in a typical morning, these could be grouped with a little thought into categories – for example calls about new UTI symptoms, earache, low mood, follow up discussions from secondary care and out of hours encounters… the list goes on. Such a list could be reviewed by the team and tabulated in such a way that all reception staff could use to record a tally over the course of a morning. A tick in the relevant box for each call about a UTI etc.
There is not a single approach to collecting such information. We need to collect meaningful data that we can use to generate hypotheses that we can refine into ideas that we can move on quickly to test. The progress of such work depends on the volume of calls, staffing levels, and our level of understanding of the process. For example, depending on the volume of calls and staffing levels we might have an opportunity to review the tally counts quickly at 08:30 that morning, and revise the list if there were calls that did not fit into a particular category. Or we might find the first attempt at collecting data overwhelming, and therefore decide on a different approach the following day – perhaps just one person collecting the tally for their calls, or every 5th call. We might decide that we have enough information from the first day, or we might want to continue for a few days because reception staff know from prior experience that there are different types of calls on different days of the week.
When we have enough data we can plot a Pareto chart – this is a special type of bar chart that orders the categories from most common to least common along the x axis, with the count along the y axis (left side), but also plotting the cumulative percentage on a second y axis (right side). This is based on the Pareto principle that 80% of consequences come from 20% of the causes (the “vital few”). So for example the majority of a GP practice’s frequent attenders will come from a relatively small group of patients. By the same principle, it is likely that many calls to a GP practice will be grouped into a relatively small number of categories (Figure 2). Some of these reasons will be well known to all, others will perhaps be a surprise to the GPs; some will be best handled by the GP practice, others may be well managed by others (e.g. Pharmacy First, optician, dentist); some may be well understood e.g. calls about stress and low mood as a consequence of pressures during lockdown, others not e.g. the first calls about “long covid”). There are QI approaches for dealing with each of these scenarios, and turning them into ideas to test.
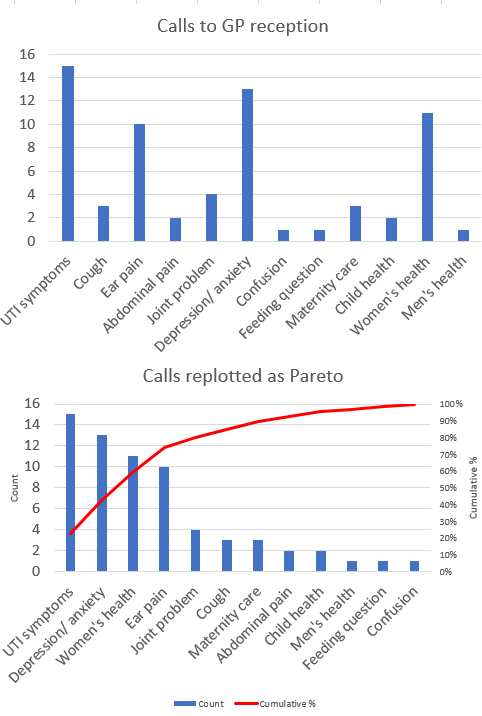
Figure 2 Made up data illustrating power of transforming data from unstructured bar chart to Pareto chart. 80% of calls are from 5 categories.
Testing ideas (PDSA cycles) is the dynamo of QI work – it challenges long-held assumptions and produces “lightbulb moments”; unpeeling the layers of understanding with each round of PDSA cycle can become irresistible. Unlike much classic audit work, such cycles of testing can be completed within a very short time frame. We should typically have 3 or 4 ideas to test, ideally spread across the team, and typically starting very small (one member of staff, one patient) – e.g. ideas for member of reception staff, GP, practice nurse, AHP. If a GP practice reception desk receives 100 phone calls between 08:00 and 08:30 then that potentially represents 100 tests. However, rather than try something out on all 100 calls, we would test an idea out for one call, with one member of staff – e.g. directing a patient to Pharmacy First for UTI symptoms. We would take a record of that patient’s CHI number and watch out for further consultations about UTI symptoms over coming days. We might call up that patient to ask about their experience.
The immediacy of testing is important – we plan, make a prediction, and ideally test against that prediction during the call or consultation, or shortly afterwards. We refine as we go – e.g. clarifying the rules for Pharmacy First and UTIs (e.g. not if pregnant, over 65 years, red flag symptoms) – before retesting.
We record measurements as we go – process measures (e.g. completeness of documentation, time per call or consultation, number of prescriptions); outcome measures (e.g. avoided hospital admissions, morbidity, mortality); balancing measures (unintended consequences including stress on colleagues measured for example by time leaving work, staff satisfaction measured by Likert scale, staff absence rates). We chart data over time, with QI charts (run charts or statistical process control charts depending on the number of time points that we have). These can plot a wide variety of measures from counts, percentages, rates, times, Likert scales. We aim to chart at the smallest level possible – so individual patient/ staff data or raw data from individual clinics rather than averages. Measurements have to be chosen carefully – e.g. a measure such as last person booked in the day risks skewing the data, just as marathon runners wearing a pantomime horse costume is not going to be representative of the marathon overall; equally a marathon run on a very windy day is going to have very odd results. We keep a record of special circumstances around data points (e.g. forthcoming Bank Holiday weekends – so called astronomical points in QI terminology).
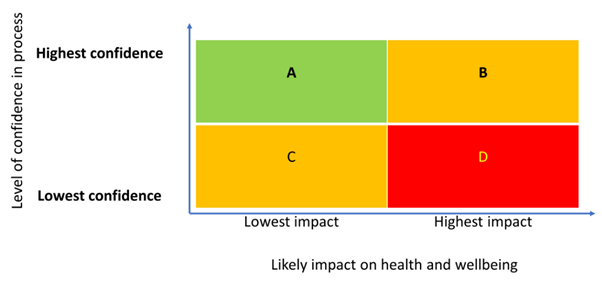
Spreading ideas and implementing change: As we identify an approach that works reliably, after comprehensive testing at individual level, we start to spread the idea so that they can be tested with the wider team. Further uncertainty and challenges are likely to emerge, requiring further refinement. When we have an approach that works across the team then we can implement the change. The speed at which we spread and implement depends on the level of certainty in the process and the likely impact on the service (Figure 3). Some changes during the pandemic may have occurred outwith such a framework, with some changes that were low confidence/ high impact for GP practices and their patients required immediately at national level for the sake of infection control and public safety.

Figure 3 Scale of test – matrix from IHI Improvement Guide.
Planning: Ideally generation and testing of ideas should be made in the context of an ambitious and patient-centred aim (e.g. patients in the GP practice area will live longer, healthier lives). Ideally this aim will also be SMART – specific, measurable, achievable, realistic and time-bound. To make something achievable we also need to remember to “think big, start small” (or on this occasion “smaller”). For example, to make an aim SMART we might need to focus on a particular patient group, age range, health condition or geographical area. For example, taking a fictional problem, if we had identified a problem with UTIs in working age adults, with higher than expected hospital admissions resulting in considerable inconvenience to patients and lost education/ work, our aim may be to reduce UTI related hospitalisations by 20% by the end of the calendar year. Such an aim would still be ambitious, but is more tangible and SMARTer.
We use driver diagrams to identify what we need to have in place to achieve such an aim (drivers). We then identify ideas to test that emerge from these drivers. Often the first “ideas to test” are too big – e.g. introduce training programme, write a policy, buy new equipment. We then go through further iterations to move from these big concepts to ideas that can be tested at an individual level. The original “idea to test” is turned into an aim and used to produce the next level of driver diagram (nesting).
For example taking the idea of staff training from our first driver diagram, we might reframe this as an aim that all staff members are knowledgeable about local services and evidence-based approaches relevant to our patients on the next level of driver diagram. Drivers for this aim might include:
- Staff knowledge (e.g. is there a directory of services, including knowledge of the Pharmacy First service for patients under 65 with UTI; and in more complicated case are there details of clinics for outpatient investigation and follow up etc);
- Evidence-base (e.g. availability of current guidance for recurrent UTIs in different age groups)
- IT approaches (e.g. reminders on Vision for specific circumstances including perhaps prescribing advice based on current microbiology surveillance)
These drivers can become ideas to test – e.g. a prompt at reception to remember Pharmacy First for eligible patients.
This “nested” approach can be represented more simply as a Russian doll. The ambitious ideas that are outwith our immediate grasp are often called “world peace” goals. If we run with that metaphor, the outer Russian doll would be world peace. Conflict between and within nations is often driven by inequalities (e.g. pressure on water, food). To achieve equality we would need to make our societies fairer and more equal. To do this we might look at taxation and benefits. Each of these ideas is well outside our grasp as clinicians, or even as directors of a health board. However the way that the benefits system is run means that clinicians may have to confirm details on an application form (e.g. GP, midwife or health visitor signature on the old Health Start scheme, now called Best Start), or patients may need additional support in the application from a link worker or welfare rights adviser. We know that benefits are underclaimed to the tune of £Billions across the UK. Work in GP practices by reception staff, midwives, health visitors and link workers could help eligible families apply for their vouchers earlier in pregnancy, reducing inequalities, and making first steps towards achieving world peace. An example of this type of work was conducted successfully in north east Edinburgh, securing £3 million previously unclaimed benefits and entitlements. The focused intervention can be conceptualised in relationship to the bigger picture (Figure 4).

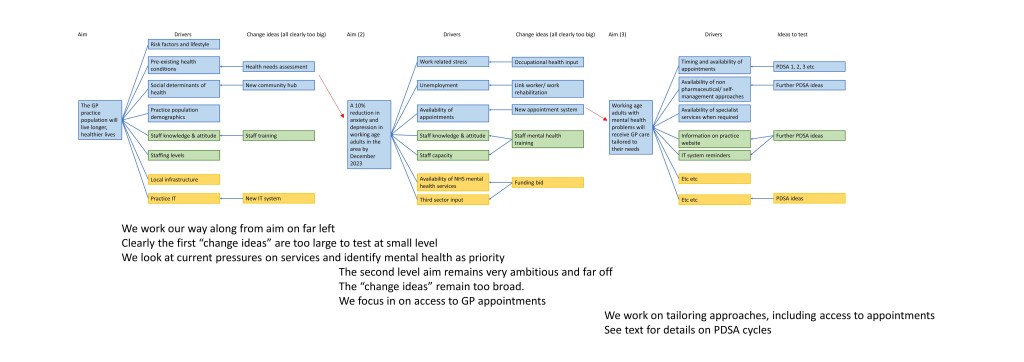
Ideally all QI work would make a driver diagram capturing their overall aim, drivers and ideas to test. However at a time of crisis, such as the Covid-19 pandemic, it might not be possible to draw this out as completely as would be desirable. It is helpful to understand the principles, and have a rough sketch, as this can help planning and ensure that there is a spread of testing across the different work in the GP practice. See appendix for a sketch of a nested driver diagram for the worked mental health example presented below (I have drafted this rapidly for illustrative purposes – ideally a driver diagram will be drawn up with input from the full team – however this can be time consuming and risks losing the enthusiasm of a team in QI work).
All QI work should also be informed by process mapping. Drawing out the processes helps identify the different steps required, but also identify areas of uncertainty. In drawing up a process map it will often become apparent that different members of a team will often have quite different views of how the process works.
The team can prioritise ideas from driver diagrams and/or process maps. Those areas that are felt to be highest impact, but where there is lowest confidence in the process, may be the first focus for testing (category D in Figure 5), though decisions also need to be informed by likely volume of testing.
Bringing it all together – a mental health example: This report has laid out the context of changes during the pandemic, thinking about future changes with loosening of lockdown, and has summarised general QI principles, putting them in a practical context. If a GP practice is considering options for moving away from booking all appointments on the day to allowing some routine appointments to be booked days and weeks in advance, QI principles could help. The following fictional example has been created to show different QI tools at work.
Tally counts and Pareto charts could be used to identify the most common reasons for calls to reception, and the issues discussed during GP telephone consultations. The GP practice team may consider that some of the most common reasons for presentation are already well managed (e.g. UTI symptoms and signposting to pharmacist). This might not therefore be a useful place to focus (though it is surprising how often expectations are confounded once testing takes place).
Once an area for testing is identified (e.g. perhaps mental health calls), ideas for testing should be developed by the team, ideally using some of the approaches introduced in the planning section above. Testing at small scale is useful as it minimises risk to patients and the GP practice. Rather than announcing a change on the GP practice recorded message or website, or introducing for all calls to the GP practice, an idea can be tested with a small number of patients, collecting information using PDSA cycles. We can see if the ideas work and are acceptable, but without setting a precedent for all patients. The following suggestions are presented solely for illustrative processes. There are clearly some conditions and presentations for such an approach would not work – e.g. a new presentation with chest pain.
Let’s say that we decide to make changes for patients calling with anxiety or low mood. Trained reception staff could ask patients calling up about anxiety/ low mood if they have had any thoughts about self harming/ suicidal ideation. If they have had such thoughts they will be booked for an appointment that day. If they haven’t had such ideas then they will be offered signposting to the GP practice webpage on mental health resources available during the Covid-19 pandemic. (To provide safety netting this includes information should the patient reach crisis point in the future and require urgent advice and support). If after reading the general information about mental health the patient phones back then they could be asked to complete PHQ-9 (depression) and GAD-7 (anxiety) questionnaires and given a telephone appointment a few days later with the GP. This approach could readily be drawn out in a process map.
We are going to take testing in small steps. The purpose of this work is to assess – starting with those patients presenting with mental health problems – whether it is feasible and acceptable to patients and staff to schedule some future appointments rather than same day appointments. The examples below focus on reception staff, but there would also be ideas to test for GPs and other members of the team.
Test 1) We ask one of the reception staff to ask the next patient that calls with anxiety/ depression whether they have had thoughts about self-harm/ suicidal ideation. The staff member predicts that the patient will be distressed to be asked this question by reception staff and is surprised when in fact they answer openly without apparent distress. For this first test we are exploring the acceptability of the question, so the patient is booked for a same day appointment.
Test 2) For the next test the staff member predicts that the patient will be happy to be signposted to the website in the first instance. The member of staff feels more confident to ask the next patient who calls about self harm/ suicidal ideation, and again there is no distress in answering the question. The patient is then asked whether they would consider self-management approaches described on the practice website rather than automatic appointment with the GP. The patient tells the reception staff member that in fact they have already read the webpage, tried out some of the options, and would prefer to move straight to the GP appointment. They would be willing to delay this for a few days. The prediction about the webpage was wrong, but it raises further ideas to test. The staff member thinks that this patient was unusual in having checked the website. She predicts that perhaps ¼ patients will have checked the website.
Test 3) The reception staff member is feeling more confident and is looking forward to checking whether the predictions are correct. When another patient phones up however the patient becomes very distressed to be asked about self harm/ suicidal ideation, expressing outrage to be asked something so personal, and stating that they will make a complaint. The reception staff member realises that this is not going to help this patient, so doesn’t push any further and slots the patient in for an appointment that day, and discusses the call with colleagues. The wording of the question about self harm/ suicidal ideation is reviewed and changed so that it is more sensitive, and gives the patient the option not to answer. If no answer is given then a same-day appointment is given. The GP practice manager is informed in case there is a patient complaint, and the GP talking to the patient later that day is able to discuss further with the patient. As we are testing the approach one patient at a time we have minimised the risk of harm to the patient and reputational damage to the GP practice. Reviewing the case everybody agrees that there was no lasting harm done and that the patient’s concerns were easily addressed. They all feel more comfortable with the reworded question and new process.
Tests 4-9) This new question is used a few more times without further difficulty. Some patients answer directly and agree to the approach described, while others prefer not to answer or state that they have had thoughts about self harm and are therefore slotted into same-day appointments. About 1/3 patients have visited the GP practice’s mental health webpage prior to their call.
Spread – tests 10-15) The approach is shared with other reception staff and tested without difficulty. The results are broadly similar after extending to colleagues.
Implementation) After discussion with the GP practice team the approach is introduced at a whole practice level and explained on the GP practice website.
Charting) Throughout the testing and implementation the results are plotted on a series of run charts for a range of process, outcome and balancing measures (a “basket of measures”). These charts show that the calls take reception staff a bit longer (~45 seconds) and this can delay answering other calls, but there has not been an increase in patients ringing off for calls overall. There has not been an increase in mental health hospitalisation/ self-harm/ suicide in the practice population. There has been a reduction in prescribing for anxiety/ depression (10%) but an increased use of computer CBT (20%) as measured by website traffic. The waiting list for counselling services has increased (now 5 months rather than 2 months). The GP practice and local voluntary sector organisation that provides counselling have put in a funding bid for another counsellor, and this bid has been successful. The funders were impressed with the availability of data to back up the bid.
Other QI data) Pareto charts and other QI methods provide methods for qualitative data collection and analysis. GPs report that more of their time in mental health consultations is spent on patient-centred issues rather than process-focused work (e.g. requesting and scoring patient questionnaires, signposting patients with mild symptoms to self-management advice on website). This is backed up by run charts looking at GP and patient satisfaction.
The practice plans to extend the approach to include other common calls amenable to such an approach. Having repeated the data collection and Pareto chart in May there are more calls about allergic rhinitis and sports injuries. Signposting to advice and pharmacy support for hayfever, and access to the practice physiotherapist are explored in further rounds of testing.
The practice takes steps to rearrange the consulting rooms to allow more face-to-face consultations, but in August 2021 a new Covid-19 variant is discovered in music fans returning from a festival in Ullapool and the UK enters its 3rd full lockdown.
Conclusions:
This introduction to QI in general practice – and the fictional data and examples included here – highlights the power of thinking big, starting small and testing fast to dissect and improve a complex system. It also reinforces the importance of ongoing data collection and testing, identifying the change in circumstances over time (e.g. for conditions such as seasonal rhinitis). QI relies on rapid data collection and testing, and is therefore ideally suited for problems that are relatively common. QI requires data collection as close as possible in time to the point of testing (typically process and balancing measures; outcome measures will take longer to collect). The testing should focus on areas of uncertainty and high impact and there should be a clear idea from process maps and driver diagrams as to how the testing links into the bigger picture of improving population health. These methods would be well suited to team working in a GP practice recovering from the impact of the Covid-19 pandemic. As also illustrated, however, sometimes huge upheaval means that these methods are not feasible, and we have to accept the attendant risks, as at the start of the pandemic.
Dr Graham Mackenzie, GPST3, Edinburgh, Scotland
28 April 2021

Appendix: An example of a nested driver diagram (3 levels). This is for illustrative purposes only. By the time we have reached the far right of the figure we have ideas that can be tested at level of individual member of staff/ individual patient during the next working day. This is the immediacy required for QI work.